
Acculturative Stress, Perceived Social Support, and Mental Health: The Mediating Effect of Negative Emotions Associated with Discrimination
 , ,
, , 
Abstract
:1. Introduction
1.1. Acculturative Stress, Emotions Associated with Discrimination, and Mental Health
1.2. The Role of Perceived Social Support in Acculturative Stress and Mental Health Symptomatology
1.3. Adaptation and Length of Residence in the Host Country
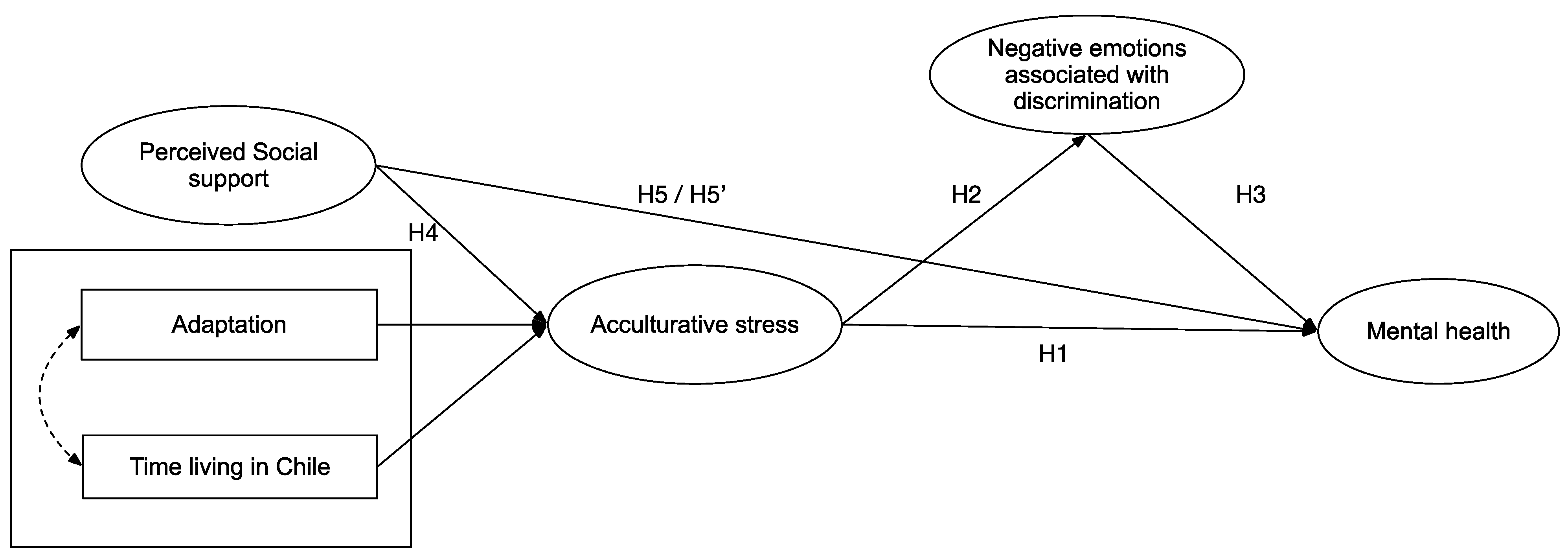
1.4. The Present Study
2. Materials and Methods
2.1. Instruments
2.1.1. Acculturative Stress
2.1.2. Negative Emotions and Affective States Associated with Discrimination
2.1.3. Mental Health Symptomatology
2.1.4. Perceived Social Support
2.1.5. Control Variables
2.2. Data Collection
2.3. Data Analysis
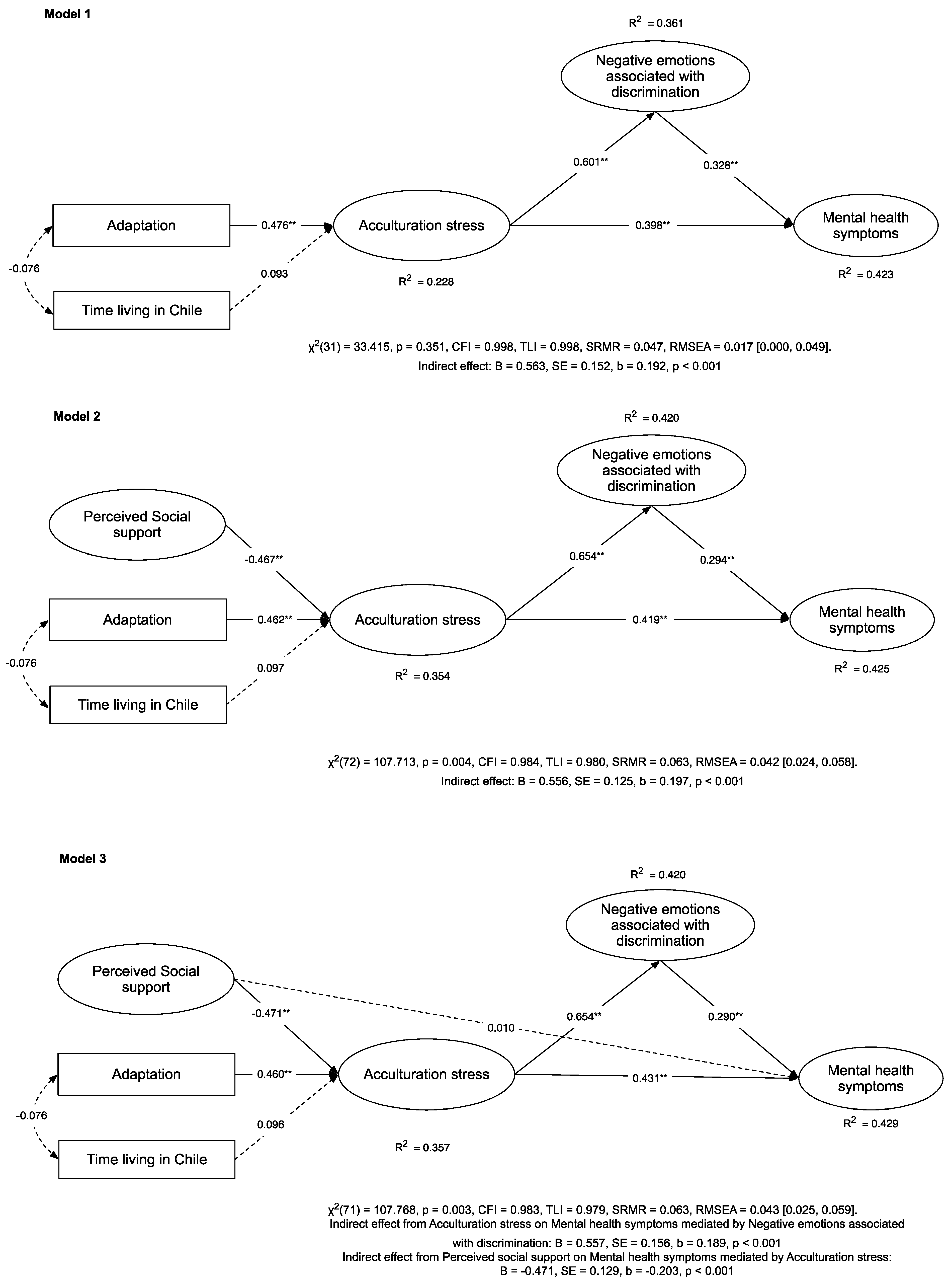
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Triandafyllidou, A. Handbook of Migration and Globalization; Edward Elgar Publishing: Cheltenham, UK, 2018. [Google Scholar]
- United Nations Department of Economic and Social Affairs. International Migrant Stock. Population Division. Available online: https://www.un.org/development/desa/pd/content/international-migrant-stock (accessed on 2 September 2022).
- International Organization for Migration. World Migration Report 2003: Managing Migration Challenges and Responses for People on the Move; International Organization for Migration: Geneva, Switzerland, 2003. [Google Scholar]
- International Organization for Migration. World Migration Report 2022; International Organization for Migration: Geneva, Switzerland, 2021. [Google Scholar]
- Cerrutti, M.; Parrado, E. Intraregional Migration in South America: Trends and a Research Agenda. Annu. Rev. Sociol. 2015, 41, 399–421. [Google Scholar] [CrossRef]
- Stefoni, C. Panorama de la Migración Internacional en América del Sur. In Documento Elaborado en el Marco de la Reunión Regional Latinoa-Mericana y Caribeña de Expertas y Expertos en Migración Internacional Preparatoria del Pacto Mundial Para una Migración Segura, Ordena; Naciones Unidas: Santiago, Chile, 2018. [Google Scholar]
- Canales, A. Estudio de las contribuciones de las migraciones recientes al desarrollo sostenible: El caso de Chile. In “Sobre las Contribuciones de la Migración al Desarrollo Sostenible: Estudios en Países Seleccionados”, Documentos de Proyectos (LC/TS.2021/195); Martínez-Pizarro, J., Cano-Christiny, M., Eds.; Comisión Económica para América Latina y el Caribe (CEPAL): Santiago, Chile, 2022; pp. 15–107. [Google Scholar]
- Valenzuela-Vergara, E. Frontera y luchas migrantes: Riesgos y desafíos en el norte de Chile. In Migraciones, Derechos Humanos y Acciones Locales; Frey, B., Forcinito, A., Pardo-Montaño, A.M., Eds.; Hispanic Issues On Line: Minneapolis, MN, USA, 2020; pp. 92–105. [Google Scholar]
- Cambero, F. Chile Anti-Migrant Protesters Destroy Camps in Tense North. Available online: https://www.reuters.com/world/americas/chile-anti-migrant-protesters-destroy-camps-tense-north-2022-01-30/ (accessed on 2 September 2022).
- Connectas. Chile Rejects the Migrants It Once Welcomed. GlobalVoice 2021. Available online: https://globalvoices.org/2021/10/19/chile-rejects-the-migrants-it-once-welcomed/ (accessed on 2 September 2022).
- National Institute of Statistics of Chile; Department of Foreigners and Migration of Chile. Estimación de Personas Extranjeras: Residentes Habituales en Chile al 31 de diciembre de 2020. Distribución Regional y Comunal; Ministry of Economy, Development and Tourism: Santiago, Chile; Ministry of the Interior and Public Security: Santiago, Chile, 2021. [Google Scholar]
- Avaria, A.; Cabieses, B.; Obach, A. Salud y Migraciones: Relevancia, Consideraciones Generales y Desafíos Para el Chile de Hoy, 1st ed.; RIL Editores: Santiago, Chile, 2021. [Google Scholar]
- Baeza-Rivera, M.J.; Salinas-Oñate, N.; Salazar-Fernández, C.; Said, J.L.; Leal, L.A. Inmigración en La Araucanía, ¿cómo viven este proceso haitianos, colombianos y venezolanos? Rev. Psicol. 2022, 31, 42–53. [Google Scholar] [CrossRef]
- Latinobarómetro. Informe Latinobarómetro Chile 1995–2020. Available online: https://www.latinobarometro.org (accessed on 2 September 2022).
- Goic, A. The Chilean health care system: The task ahead. Rev. Med. Chil. 2015, 143, 774–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Organization for Migration. Migration and the 2030 Agenda; International Organization for Migration: Geneva, Switzerland, 2018. [Google Scholar]
- Urzúa, A.; Vega, M.; Jara, A.; Trujillo, S.; Muñoz, R.; Caqueo-Urízar, A. Calidad de vida percibida en inmigrantes sudamericanos en el norte de Chile. Ter. Psicol. 2015, 33, 139–156. [Google Scholar] [CrossRef] [Green Version]
- Rojas, G.; Fritsch, R.; Castro, A.; Guajardo, V.; Torres, P.; Díaz, B. Trastornos mentales comunes y uso de servicios de salud en población inmigrante. Rev. Med. De Chile 2011, 139, 1298–1304. [Google Scholar] [CrossRef]
- Lindert, J.; Schouler-Ocak, M.; Heinz, A.; Priebe, S. Mental health, health care utilisation of migrants in Europe. Eur. Psychiatry 2008, 23, s114–s120. [Google Scholar] [CrossRef]
- Carroll, H.; Luzes, M.; Freier, L.F.; Bird, M. The migration journey and mental health: Evidence from Venezuelan forced migration. SSM Popul. Health 2020, 10, 100551. [Google Scholar] [CrossRef]
- Fuster, F.; Peirano, F.; Vargas, J.I.; Zamora, F.X.; López-Lastra, M.; Núñez, R.; Soza, J.; González, K.; Estay, D.; Barchiesi, B.; et al. Infectious and non-infectious diseases burden among Haitian immigrants in Chile: A cross-sectional study. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Berry, J.W. Acculturation: Living successfully in two cultures. Int. J. Intercult. Relations 2005, 29, 697–712. [Google Scholar] [CrossRef]
- Schwartz, S.J.; Unger, J.B.; Zamboanga, B.L.; Szapocznik, J. Rethinking the concept of acculturation: Implications for theory and research. Am. Psychol. 2010, 65, 237–251. [Google Scholar] [CrossRef]
- Cavazos-Rehg, P.; Zayas, P.; Spitznagel, E. Acculturative Stress Among Documented and Undocumented Latino Immigrants in the United States. Hisp. J. Behav. Sci. 2010, 32, 362–384. [Google Scholar] [CrossRef]
- Berry, J. Globalisation and acculturation. Int. J. Intercult. Relations 2008, 32, 328–336. [Google Scholar] [CrossRef]
- Urzúa, A.; Basabe, N.; Pizarro, J.J.; Ferrer, R. Afrontamiento del estrés por aculturación: Inmigrantes latinos en Chile. Univ. Psychol. 2018, 16, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Urzúa, A.; Heredia, O.; Caqueo-Urízar, A. Salud mental y estrés por aculturación en inmigrantes sudamericanos en el norte de Chile. Rev. Médica Chile 2016, 144, 563–570. [Google Scholar] [CrossRef] [Green Version]
- Mera-Lemp, M.J.; Martínez-Zelaya, G.; Orellana, A.; Smith-Castro, V. Orientaciones de aculturación, estrés de aculturación y bienestar psicológico en inmigrantes latinoamericanos en Santiago de Chile. Acta. Colomb. De Psicol. 2020, 23, 216–230. [Google Scholar] [CrossRef] [Green Version]
- Urzúa, A.; Leiva-Gutiérrez, J.; Caqueo-Urízar, A.; Vera-Villarroel, P. Rooting mediates the effect of stress by acculturation on the psychological well-being of immigrants living in Chile. PLoS ONE 2019, 14, e0219485. [Google Scholar] [CrossRef] [Green Version]
- Silva, J.; Urzúa, A.; Caqueo-Urízar, A.; Lufin, M.; Irarrazabal, M. Bienestar psicológico y estrategias de aculturación en in-migrantes afrocolombianos en el norte de Chile. Interciencia 2016, 41, 804–811. [Google Scholar]
- Waldman, K.; Koyanagi, A.; Wang, J.S.-H.; Ko, J.; DeVylder, J.; Oh, H. Acculturative stress, disability, and health treatment utilization among Asian and Latin American immigrants in the United States. Soc. Psychiatry 2019, 54, 1275–1284. [Google Scholar] [CrossRef]
- Choy, B.; Arunachalam, K.; Gupta, S.; Taylor, M.; Lee, A. Systematic review: Acculturation strategies and their impact on the mental health of migrant populations. Public Health Pract. 2020, 2, 100069. [Google Scholar] [CrossRef]
- Ugalde-Watson, K.; Smith-Castro, V.; Moreno-Salas, M.; Rodríguez-García, J.M. Estructura, correlatos y predictores del estrés por Aculturación. El caso de personas refugiadas colombianas en Costa Rica. Univ. Psychol. 2010, 10, 759–774. [Google Scholar] [CrossRef] [Green Version]
- Fajardo, M.; Patiño, M.; Patiño, C. Estudios actuales sobre aculturación y salud mental en inmigrantes: Revisión y perspectivas. Rev. Iberoam. De Psicol. Cienc. Y Tecnol. 2008, 1, 39–50. [Google Scholar]
- Sánchez, G.; López, M. Ansiedad y modos de aculturación en la población inmigrante. Apunt. Psicol. 2008, 26, 399–410. [Google Scholar]
- Bekteshi, V.; Van Hook, M. Contextual Approach to Acculturative Stress Among Latina Immigrants in the U.S. J. Immigr. Minor. Health 2015, 17, 1401–1411. [Google Scholar] [CrossRef] [PubMed]
- Torrealba, S.B.; Caqueo-Urízar, A. Salud mental y estrategias de aculturación en inmigrantes colombianos y peruanos en el Norte de Chile. Acta Colomb. De Psicol. 2017, 20, 70–89. [Google Scholar] [CrossRef]
- Bekteshi, V.; Kang, S.-W. Contextualizing acculturative stress among Latino immigrants in the United States: A systematic review. Ethn. Health 2020, 25, 897–914. [Google Scholar] [CrossRef]
- Tartakovsky, E. A longitudinal study of acculturative stress and homesickness: High-school adolescents immigrating from Russia and Ukraine to Israel without parents. Soc. Psychiatry 2007, 42, 485–494. [Google Scholar] [CrossRef]
- Gómez-Pérez, D.; Salinas-Rehbein, B.; Becerra-Muñoz, C.; Ortiz, M.S. Percepción de Discriminación y Obesidad: El Rol de la Afectividad Negativa y la Calidad de la Dieta. Psykhe 2021, 30, 1–11. [Google Scholar] [CrossRef]
- Zeiders, K.H.; Doane, L.; Roosa, M.W. Perceived discrimination and diurnal cortisol: Examining relations among Mexican American adolescents. Horm. Behav. 2012, 61, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Pascoe, E.A.; Smart Richman, L. Perceived discrimination and health: A meta-analytic review. Psychol. Bull. 2009, 135, 531–554. [Google Scholar] [CrossRef] [Green Version]
- Smith-Castro, V. Experiencias de discriminación social de inmigrantes nicaragüenses En Costa Rica: Reacciones afectivas y atribuciones causales. Interam. J. Psychol. 2010, 44, 368–381. [Google Scholar]
- Ortiz, M.S.; Baeza-Rivera, M.J.; Salinas-Oñate, N.; Flynn, P.; Betancourt, H. Atribución de malos tratos en servicios de salud a discriminación y sus consecuencias en pacientes diabéticos mapuche. Rev. Med. Chil. 2016, 144, 1270–1276. [Google Scholar] [CrossRef] [Green Version]
- Baeza-Rivera, M.J.; Betancourt, H.; Salinas-Oñate, N.; Ortiz, M.S. Creencias culturales sobre los médicos y percepción de discriminación: El impacto en la continuidad de la atención. Rev. Med. De Chile 2019, 147, 161–167. [Google Scholar] [CrossRef] [Green Version]
- Baeza-Rivera, M.J. Discriminación Percibida y sus Consecuencias en las Conductas de Cuidado de la salud: Un Estudio Multifactorial. Ph.D. Thesis, Universidad de La Frontera, Temuco, Chile, 2015. [Google Scholar]
- Flynn, P.M.; Betancourt, H.; Ormseth, S.R. Culture, Emotion, and Cancer Screening: An Integrative Framework for Investigating Health Behavior. Ann. Behav. Med. 2011, 42, 79–90. [Google Scholar] [CrossRef] [Green Version]
- Flynn, P.M.; Betancourt, H.; Garberoglio, C.; Regts, G.J.; Kinworthy, K.M.; Northington, D.J. Attributions and emotions regarding health care mistreatment impact continuity of care among Latino and Anglo American women. Cult. Divers. Ethn. Minor. Psychol. 2015, 21, 593–603. [Google Scholar] [CrossRef]
- Fleming, P.J.; Villa-Torres, L.; Taboada, A.; Richards, C.; Barrington, C. Marginalisation, discrimination and the health of Latino immigrant day labourers in a central North Carolina community. Health Soc. Care Community 2017, 25, 527–537. [Google Scholar] [CrossRef] [Green Version]
- De Leersnyder, J.; Mesquita, B.; Kim, H.S. Where Do My Emotions Belong? A Study of Immigrants’ Emotional Acculturation. Pers. Soc. Psychol. Bull. 2011, 37, 451–463. [Google Scholar] [CrossRef] [Green Version]
- Consedine, N.S.; Chentsova-Dutton, Y.E.; Krivoshekova, Y.S. Emotional Acculturation Predicts Better Somatic Health: Experiential and Expressive Acculturation Among Immigrant Women From Four Ethnic Groups. J. Soc. Clin. Psychol. 2014, 33, 867–889. [Google Scholar] [CrossRef]
- Mesquita, B.; Boiger, M.; De Leersnyder, J. The cultural construction of emotions. Curr. Opin. Psychol. 2016, 8, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Mayorga, N.A.; Jardin, C.; Bakhshaie, J.; Garey, L.; Viana, A.G.; Cardoso, J.B.; Zvolensky, M. Acculturative stress, emotion regulation, and affective symptomology among Latino/a college students. J. Couns. Psychol. 2018, 65, 247–258. [Google Scholar] [CrossRef]
- Cheung, R.Y.M.; Bhowmik, M.K.; Hue, M.-T. Why does acculturative stress elevate depressive symptoms? A longitudinal study with emotion regulation as a mediator. J. Couns. Psychol. 2020, 67, 645–652. [Google Scholar] [CrossRef]
- Lin, N.; Dean, A.; Ensel, W. Social Support, Life Events, and Depression; Academic Press: Orlando, FL, USA, 1986. [Google Scholar]
- Canty-Mitchell, J.; Zimet, G. Psychometric Properties of the Multidimensional Scale of Perceived Social Support in Urban Adolescents. Am. J. Community Psychol. 2000, 28, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Persinal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Hashemi, N.; Marzban, M.; Sebar, B.; Harris, N. Perceived discrimination and subjective well-being among Middle Eastern migrants in Australia: The moderating role of perceived social support. Int. J. Soc. Psychiatry 2021, 67, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Batz-Barbarich, C.; Tay, L.; Kuykendall, L.; Cheung, H.K. A Meta-Analysis of Gender Differences in Subjective Well-Being: Estimating Effect Sizes and Associations with Gender Inequality. Psychol. Sci. 2018, 29, 1491–1503. [Google Scholar] [CrossRef] [PubMed]
- Wachter, K.; Bunn, M.; Schuster, R.C.; Boateng, G.O.; Cameli, K.; Johnson-Agbakwu, C.E. A Scoping Review of Social Support Research among Refugees in Resettlement: Implications for Conceptual and Empirical Research. J. Refug. Stud. 2021, 35, 368–395. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S. Social Relationships and Health. Am. Psychol. 2004, 59, 676–684. [Google Scholar] [CrossRef]
- Itzick, M.; Kagan, M.; Tal-Katz, P. Perceived social support as a moderator between perceived discrimination and subjective well-being among people with physical disabilities in Israel. Disabil. Rehabilitation 2018, 40, 2208–2216. [Google Scholar] [CrossRef]
- Khatiwada, J.; Muzembo, B.A.; Wada, K.; Ikeda, S. The effect of perceived social support on psychological distress and life satisfaction among Nepalese migrants in Japan. PLoS ONE 2021, 16, e0246271. [Google Scholar] [CrossRef]
- Koskinen, M.; Elovainio, M.; Raaska, H.; Sinkkonen, J.; Matomäki, J.; Lapinleimu, H. Perceived racial/ethnic discrimination and psychological outcomes among adult international adoptees in Finland: Moderating effects of social support and sense of coherence. Am. J. Orthopsychiatry 2015, 85, 550–564. [Google Scholar] [CrossRef] [Green Version]
- Puyat, J.H. Is the Influence of Social Support on Mental Health the Same for Immigrants and Non-Immigrants? J. Immigr. Minor. Health 2013, 15, 598–605. [Google Scholar] [CrossRef]
- Seawell, A.H.; Cutrona, C.E.; Russell, D. The Effects of General Social Support and Social Support for Racial Discrimination on African American Women’s Well-Being. J. Black Psychol. 2014, 40, 3–26. [Google Scholar] [CrossRef] [Green Version]
- Umberson, D.; Crosnoe, R.; Reczek, C. Social Relationships and Health Behavior Across the Life Course. Annu. Rev. Sociol. 2010, 36, 139–157. [Google Scholar] [CrossRef] [Green Version]
- Villarroel, P.; De La Frontera, U.; Ortiz, M.S. Social negativity and obesity: Role of negative affectivity. Rev. Argent. DE Clin. Psicol. 2019, 28, 744. [Google Scholar] [CrossRef]
- Mora-Guerrero, G.M.; Escárate-Colín, L.M.; Espinoza-Lerdón, C.A.; Peña-Paredes, A.B. Apoyo social percibido, autoestima y maternidad adolescente: Entre el respeto y la intrusión. Estudio en Traiguén, Chile. Prospectiva 2021, 32, 151–171. [Google Scholar] [CrossRef]
- Dutton, Y.E.C. Butting In vs. Being a Friend: Cultural Differences and Similarities in the Evaluation of Imposed Social Support. J. Soc. Psychol. 2012, 152, 493–509. [Google Scholar] [CrossRef]
- Goldsmith, D.J. Communicating Social Support; Cambridge University Press: Cambridge, UK, 2004. [Google Scholar] [CrossRef]
- Harber, K.D.; Schneider, J.K.; Everard, K.M.; Fisher, E.B. Directive Support, Nondirective Support, and Morale. J. Soc. Clin. Psychol. 2005, 24, 691–722. [Google Scholar] [CrossRef]
- Reinhardt, J.P.; Boerner, K.; Horowitz, A. Good to have but not to use: Differential impact of perceived and received support on well-being. J. Soc. Pers. Relationships 2006, 23, 117–129. [Google Scholar] [CrossRef]
- Ibarra-Rovillard, M.S.; Kuiper, N.A. Social support and social negativity findings in depression: Perceived responsiveness to basic psychological needs. Clin. Psychol. Rev. 2011, 31, 342–352. [Google Scholar] [CrossRef]
- Espinoza, M.D.C.; Gavidia-Payne, S.; Okumura, A. Understanding emotion regulation in Venezuelan immigrants to Peru and Peruvian internal migrants: A comparative study. J. Ethn. Migr. Stud. 2021, 1–22. [Google Scholar] [CrossRef]
- Khan, A.; Hasan, B. Moderating effect of social support on the link between acculturation experiences and acculturative stress. Int. J. Soc. Sci. 2019, 7, 1775–1781. [Google Scholar]
- Ye, J. An Examination of Acculturative Stress, Interpersonal Social Support, and Use of Online Ethnic Social Groups among Chinese International Students. Howard J. Commun. 2006, 17, 1–20. [Google Scholar] [CrossRef]
- Yeh, C.J.; Inose, M. International students’ reported English fluency, social support satisfaction, and social connectedness as predictors of acculturative stress. Couns. Psychol. Q. 2003, 16, 15–28. [Google Scholar] [CrossRef]
- Chae, S.-M.; Park, J.W.; Kang, H.S. Relationships of Acculturative Stress, Depression, and Social Support to Health-Related Quality of Life in Vietnamese Immigrant Women in South Korea. J. Transcult. Nurs. 2014, 25, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Amason, P.; Allen, M.W.; Holmes, S.A. Social support and acculturative stress in the multicultural workplace. J. Appl. Commun. Res. 1999, 27, 310–334. [Google Scholar] [CrossRef]
- Nandi, A.; Galea, S.; Lopez, G.; Nandi, V.; Strongarone, S.; Ompad, D.C. Access to and Use of Health Services Among Undocumented Mexican Immigrants in a US Urban Area. Am. J. Public Health 2008, 98, 2011–2020. [Google Scholar] [CrossRef]
- Arcury, T.A.; Quandt, S.A. Delivery of Health Services to Migrant and Seasonal Farmworkers. Annu. Rev. Public Health 2007, 28, 345–363. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-J.; Hong, S.; Kim, M. Living Arrangement, Social Connectedness, and Life Satisfaction among Korean Older Adults with Physical Disabilities: The Results from the National Survey on Persons with Disabilities. J. Dev. Phys. Disabil. 2014, 27, 307–321. [Google Scholar] [CrossRef]
- Martínez-García, M.; García-Ramírez, M.; Maya-Jariego, I. El efecto amortiguador del apoyo social sobre la depresión en un colectivo de inmigrantes. Psicothema 2001, 13, 605–610. [Google Scholar]
- Jang, S.; Go, J. Relationship between acculturative stress and mental health of multicultural youths. Focused on the mediating effect of social support. J. Korea Contents Assoc. 2021, 21, 662–673. [Google Scholar]
- Papadopoulos, I.; Lees, S.; Lay, M.; Gebrehiwot, A. Ethiopian refugees in the UK: Migration, adaptation and settlement experiences and their relevance to health. Ethn. Health 2004, 9, 55–73. [Google Scholar] [CrossRef]
- Bhugra, D.; Gupta, S.; Schouler-Ocak, M.; Graeff-Calliess, I.; Deakin, N.A.; Qureshi, A.; Dales, J.; Moussaoui, D.; Kastrup, M.; Tarricone, I.; et al. EPA Guidance Mental Health Care of Migrants. Eur. Psychiatry 2014, 29, 107–115. [Google Scholar] [CrossRef]
- Ghaffarian, S. The Acculturation of Iranian Immigrants in the United States and the Implications for Mental Health. J. Soc. Psychol. 1998, 138, 645–654. [Google Scholar] [CrossRef]
- Cabieses, B.; Tunstall, H.; Pickett, K. Testing the Latino paradox in Latin America: A population-based study of Intra-regional immigrants in Chile. Rev. Med. Chil. 2013, 141, 1255–1265. [Google Scholar] [CrossRef] [Green Version]
- Maskileyson, D.; Seddig, D.; Davidov, E. The Comparability of Perceived Physical and Mental Health Measures Across Immigrants and Natives in the United States. Demography 2021, 58, 1423–1443. [Google Scholar] [CrossRef]
- Rojas, G. Diagnóstico y Factibilidad Global para la Implementación de Políticas Globales de Salud Mental para Inmigrantes de la Zona Norte de la Región Metropolitana; Psychiatric Clinic of the University of Chile: Santiago, Chile, 2008. [Google Scholar]
- Riosmena, F.; Dennis, J.A. A Tale of Three Paradoxes: The Weak Socioeconomic Gradients in Health Among Hispanic Immigrants and Their Relation to the Hispanic Health Paradox and Negative Acculturation. In Aging, Health, and Longevity in the Mexican-Origin Population; Springer: Boston, MA, USA, 2012; pp. 95–110. [Google Scholar] [CrossRef]
- Hamilton, T.G. The healthy immigrant (migrant) effect: In search of a better native-born comparison group. Soc. Sci. Res. 2015, 54, 353–365. [Google Scholar] [CrossRef]
- Holz, M. Health inequalities in Germany: Differences in the ‘Healthy migrant effect’ of European, non-European and internal migrants. J. Ethn. Migr. Stud. 2021, 48, 2620–2641. [Google Scholar] [CrossRef]
- Nieden, F.Z.; Sommer, B. Lebenserwartung in Deutschland auf Basis des Zensus 2011: War der Healthy-Migrant-Effekt nur ein Artefakt? Comp. Popul. Stud. 2017, 41, 35–65. [Google Scholar] [CrossRef]
- Cagney, K.A.; Browning, C.R.; Wallace, D.M. The Latino Paradox in Neighborhood Context: The Case of Asthma and Other Respiratory Conditions. Am. J. Public Health 2007, 97, 919–925. [Google Scholar] [CrossRef]
- Horton, S.B.; Barker, J.C. A latino oral health paradox? using ethnography to specify the biocultural factors behind epidemiological models. NAPA Bull. 2010, 34, 68–83. [Google Scholar] [CrossRef] [Green Version]
- Nesterko, Y.; Turrión, C.M.; Friedrich, M.; Glaesmer, H. Trajectories of health-related quality of life in immigrants and non-immigrants in Germany: A population-based longitudinal study. Int. J. Public Health 2018, 64, 49–58. [Google Scholar] [CrossRef]
- Boulogne, R.; Jougla, E.; Breem, Y.; Kunst, A.E.; Rey, G. Mortality differences between the foreign-born and locally-born population in France (2004–2007). Soc. Sci. Med. 2012, 74, 1213–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhugra, D.; Gupta, S. Culture and Its Influence on Diagnosis and Management. In Principles of Social Psychiatry; Morgan, C., Bhugra, D., Eds.; John Wiley and Sons: Hoboken, NJ, USA, 2010; pp. 117–131. [Google Scholar] [CrossRef]
- Cabieses, B.; Obach, A.; Urrutia, C. Interculturalidad en Salud. teorías y Experiencias Para Poblaciones Migrantes Internacionales; Universidad del Desarrollo: Concepción, Chile, 2021. [Google Scholar]
- National Institute of Statistics of Chile. Radiografía de Género: Pueblos Originarios en Chile 2017; Ministry of Economy, Development and Tourism. Location: Santiago, Chile, 2018. [Google Scholar]
- Foerster, R.; Vergara, J.I. Etnia y nación en la lucha por el reconocimiento. Los mapuches en la sociedad chilena. Estud. Atacameños 2000, 19, 11–42. [Google Scholar] [CrossRef] [Green Version]
- Norbeck, J.S.; Tilden, V.P. International nursing research in social support: Theoretical and methodological issues. J. Adv. Nurs. 1988, 13, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Sato, Y. Relationships of Social Support, Stress, and Health among Immigrant Chinese Women in Japan: A Cross-Sectional Study Using Structural Equation Modeling. Healthcare 2021, 9, 258. [Google Scholar] [CrossRef] [PubMed]
- Tomás-Sábado, J.; Antonin, M.; Qureshi, A.; Collazos, F. Construction and Preliminary Validation of the Barcelona Immigration Stress Scale. Psychol. Rep. 2007, 100, 1013–1023. [Google Scholar] [CrossRef]
- Hernández, J.A.R.; Hernández, G.T.; González, A.R. Acculturative stress in Latin-American immigrants: An assessment proposal. Span. J. Psychol. 2011, 14, 227–236. [Google Scholar] [CrossRef]
- Antúnez, Z.; Vinet, E.V. Escalas de Depresión, Ansiedad y Estrés (DASS-21): Validación de la Versión abreviada en Estudiantes Universitarios Chilenos. Ter. Psicol. 2012, 30, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Revelle, W.; Zinbarg, R.E. Coefficients Alpha, Beta, Omega, and the glb: Comments on Sijtsma. Psychometrika 2009, 74, 145–154. [Google Scholar] [CrossRef]
- Rosseel, Y. lavaan: AnRPackage for Structural Equation Modeling. Br. J. Math. Stat. Psychol. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Team RC. A language and Environment for Statistical Computing; R Foundation for Statistical Computing R: Vienna, Austria, 2020. [Google Scholar]
- Flora, D.B.; Curran, P.J. An Empirical Evaluation of Alternative Methods of Estimation for Confirmatory Factor Analysis With Ordinal Data. Psychol. Methods 2004, 9, 466–491. [Google Scholar] [CrossRef] [Green Version]
- Marsh, H.W.; Hau, K.-T.; Wen, Z. In search of golden rules: Comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) Findings. Struct. Equ. Model. A Multidiscip. J. 2004, 11, 320–341. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating Goodness-of-Fit Indexes for Testing Measurement Invariance. Struct. Equ. Model. Multidiscip. J. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Porter, M.; Haslam, N. Predisplacement and Postdisplacement Factors Associated With Mental Health of Refugees and Internally Displaced Persons. JAMA 2005, 294, 602–612. [Google Scholar] [CrossRef]
- Grüsser, S.M.; Wölfling, K.; Mörsen, C.P.; Albrecht, U.; Heinz, A. Immigration-associated variables and substance dependence. J. Stud. Alcohol 2005, 66, 98–104. [Google Scholar] [CrossRef]
- Sieberer, M.; Maksimović, S.; Ersöz, B.; Machleidt, W.; Ziegenbein, M.; Calliess, I.T. Depressive symptoms in first-and second-generation migrants: A cross-sectional study of a multi-ethnic working population. Int. J. Soc. Psychiatry 2012, 58, 605–613. [Google Scholar] [CrossRef]
- De Leersnyder, J.; Boiger, M.; Mesquita, B. Cultural regulation of emotion: Individual, relational, and structural sources. Front. Psychol. 2013, 4, 55. [Google Scholar] [CrossRef] [Green Version]
- Hwang, H.; Matsumoto, D. Functions of emotions. In Noba Textbook Series: Psychology; Biswas-Diener, R., Diener, E., Eds.; DEF Publishers: Champaign, IL, USA, 2022; pp. 1–24. [Google Scholar]
- Urzúa, A.; Caqueo-Urízar, A.; Carvajal, C.; Páez, L. ¿El apoyo social mediatiza el efecto negativo del estrés por aculturación en la salud? Un estudio en colombianos y peruanos inmigrantes en el norte de Chile. Interciencia 2017, 42, 818–822. [Google Scholar]
- Cabieses, B.; Bernales, M.; McIntyre, A. International Migration as a Social Determinant of Health in Chile: Evidence and Recomendations for Public Policies; Universidad del Desarrollo: Santiago, Chile, 2017. [Google Scholar]
- Acevedo-Garcia, D.; Sanchez-Vaznaugh, E.V.; Viruell-Fuentes, E.A.; Almeida, J. Integrating social epidemiology into immigrant health research: A cross-national framework. Soc. Sci. Med. 2012, 75, 2060–2068. [Google Scholar] [CrossRef]
- Garcia, J.I.R. Mental Health Care for Latino Immigrants in the U.S.A. and the Quest for Global Health Equities. Psychosoc. Interv. 2012, 21, 305–318. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Riveros, C.; Urzúa, A.; Macaya-Aguirre, G.; Cabieses, B. Meanings and Practices in Intercultural Health for International Migrants. Int. J. Environ. Res. Public Health 2022, 19, 13670. [Google Scholar] [CrossRef]
- Thoits, P.A. Mechanisms Linking Social Ties and Support to Physical and Mental Health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Age | |
| Mean (standard deviation) | 34.40 (9.53) |
| Country of origin | |
| Colombia | 36 (13%) |
| Venezuela | 235 (83%) |
| Haiti | 12 (4%) |
| Marital status | |
| Single | 135 (47%) |
| Married | 69 (24%) |
| Divorced | 7 (2%) |
| De facto separated | 8 (3%) |
| Cohabiting | 64 (23%) |
| Sex | |
| Female | 189 (67%) |
| Male | 94 (33%) |
| Socioeconomic status | |
| Low, very low | 158 (55%) |
| Medium | 120 (42%) |
| High, very high | 5 (3%) |
| Level of education | |
| Complete secondary education or below | 84 (30%) |
| Complete or incomplete undergraduate education | 177 (62%) |
| Postgraduate education | 22 (8%) |
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Time living in Chile | - | |||||
| 2. Adaptation difficulties | −0.084 | - | ||||
| 3. Perceived social support | −0.037 | −0.175 * | - | |||
| 4. Acculturative stress | −0.033 | 0.389 * | −0.248 * | - | ||
| 5. Negative emotions associated with discrimination | 0.137 * | 0.254 * | −0.259 * | 0.460 * | - | |
| 6. Mental health symptoms | −0.040 | 0.265 * | −0.220 | 0.423 * | 0.502 * | - |
| Mean (SD) | 32.131 (22.460) | 3.795 (1.530) | 3.330 (1.020) | 2.480 (0.658) | 2.880 (0.840) | 2.424 (0.957) |
| Model | df | CFI | TLI | RMSEA (90% CI) | SRMR | Model Comparison | ∆CFI | |
|---|---|---|---|---|---|---|---|---|
| Model 1 | 33.415 | 31 | 0.998 | 0.998 | 0.017 (0.000, 0.049) | 0.047 | - | - |
| Model 2 | 107.713 * | 72 | 0.984 | 0.980 | 0.042 (0.024, 0.058) | 0.063 | Model 2 vs. Model 1 | −0.014 |
| Model 3 | 107.768 * | 71 | 0.983 | 0.979 | 0.043 (0.025, 0.059) | 0.063 | Model 3 vs. Model 2 | −0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baeza-Rivera, M.J.; Salazar-Fernández, C.; Manríquez-Robles, D.; Salinas-Oñate, N.; Smith-Castro, V. Acculturative Stress, Perceived Social Support, and Mental Health: The Mediating Effect of Negative Emotions Associated with Discrimination. Int. J. Environ. Res. Public Health 2022, 19, 16522. https://doi.org/10.3390/ijerph192416522
Baeza-Rivera MJ, Salazar-Fernández C, Manríquez-Robles D, Salinas-Oñate N, Smith-Castro V. Acculturative Stress, Perceived Social Support, and Mental Health: The Mediating Effect of Negative Emotions Associated with Discrimination. International Journal of Environmental Research and Public Health. 2022; 19(24):16522. https://doi.org/10.3390/ijerph192416522
Chicago/Turabian StyleBaeza-Rivera, María José, Camila Salazar-Fernández, Diego Manríquez-Robles, Natalia Salinas-Oñate, and Vanessa Smith-Castro. 2022. "Acculturative Stress, Perceived Social Support, and Mental Health: The Mediating Effect of Negative Emotions Associated with Discrimination" International Journal of Environmental Research and Public Health 19, no. 24: 16522. https://doi.org/10.3390/ijerph192416522